Improve Lives, Prevent Deaths
How to Develop a Comprehensive Approach to Prevent Overdose Deaths and Improve the Health of People Who Use Opioids
Overdose deaths and opioid use disorder continue to affect people in Washington State. Communities have made significant efforts to address this issue, though building a comprehensive and successful approach can be challenging. Fortunately, there is strong evidence about which strategies are most likely to be effective toward these goals. A comprehensive response braids multiple strategies to develop holistic supports for people with different needs.
This guide highlights actionable strategies that work and their evidence base. It also describes how to integrate these strategies within a comprehensive framework to address the holistic health needs, including overdose care, of people who use drugs.
Specific topics include:
- Evidence-based strategies
- Priority populations and settings
- Creating a holistic Opioid Overdose Response plan
- Evaluation metrics
- Examples of essential and innovative programs
- Examples of existing opioid/stimulant response plans
- Resources
Integrating Overdose Prevention and Health Promotion

Every community will benefit from a coordinated approach that maximizes short, medium, and long-term objectives to reduce the potential harms of opioids. While these strategies may differ across communities, the common goal is to connect people, organizations, and communities to maximize impact. This includes efforts to:
- Connect people to the services they need.
- Provide services where people are and make them easy to get.
- Give people information they need to make healthier decisions, while recognizing social and environmental factors that can interfere with the ability to make these decisions.
- Support staff and volunteers doing this work through training, ongoing education, and implementation support.
- Engage communities and people most affected by overdose in planning and implementation.
Evidence-based strategies
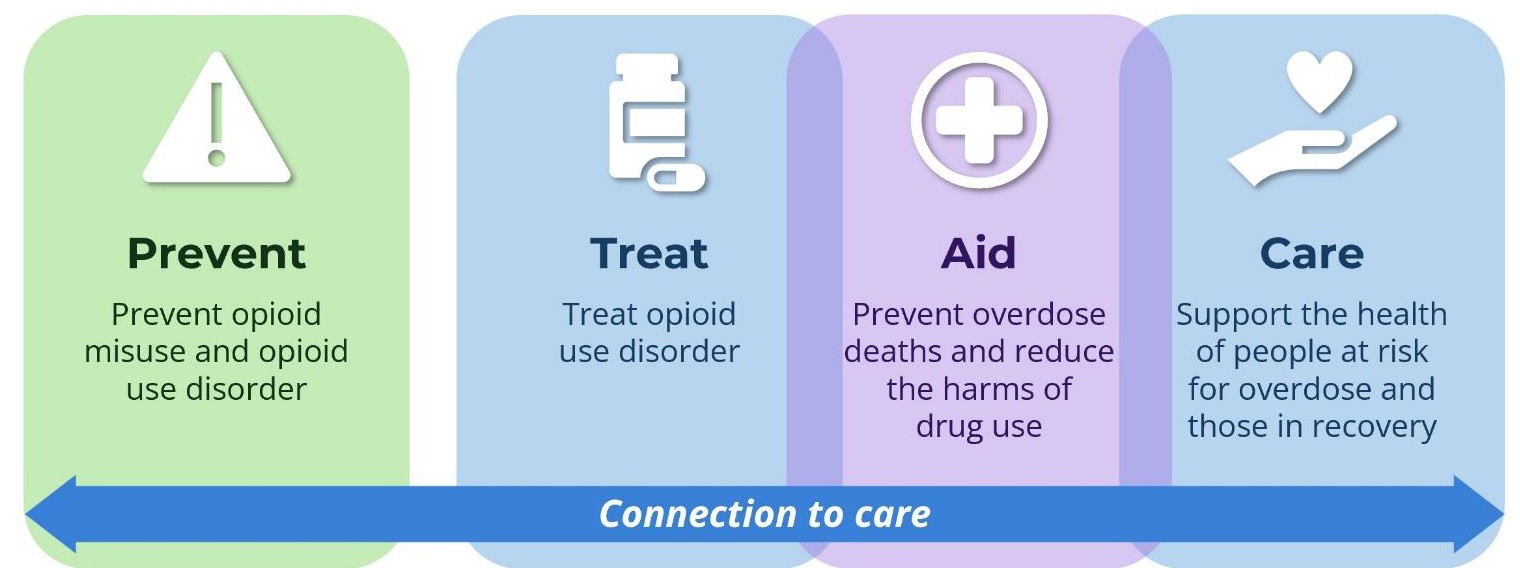
A comprehensive opioid response plan should include evidence-based strategies from each of these domains:
Multiple guides for overdose response planning include these strategies, which have been identified through a review of the scientific literature. Review the resources at the end of this document to learn more and to find a planning checklist. Keep in mind that the evidence base has often been developed in particular settings for particular populations, typically in traditional care settings and among dominant culture participants. Evidence-based interventions in one setting may not translate to another setting perfectly.
PREVENT: Prevent misuse of opioids and opioid use disorder
These strategies seek to prevent substance use/misuse, particularly among young people.* Examples include:
- Safer opioid prescribing
- Safe storage and disposal of medications
- Health care to treat physical pain and sleep issues
- Targeted youth substance use education
- Coping skills education
- Mental health supports for youth and young adults
*While trauma often plays a central role in substance use disorder, strategies to prevent and treat trauma are beyond the scope of this document.
TREAT: Treat opioid use disorder and stimulant use disorder
The gold standard of opioid use disorder (OUD) treatment is use of the medications buprenorphine and methadone. These two medications have been shown to reduce deaths from opioid use by 50% among those with opioid use disorder. For some, social supports and counseling are also helpful. Important treatment approaches include:
- Low-barrier access to buprenorphine and methadone
- Continued access to substance use disorder (SUD) treatment, even if a person has not yet stopped all substance use
- Evidence-based SUD counseling
- Treatments for stimulant use disorder including related mental health conditions
- Health care supports for those using stimulants to reduce hazards to oral, physical, and mental health
- Support groups, recovery cafes, and other social supports
Not everyone who uses opioids feels ready for or is interested in these options. Some may also need treatment and/or health care supports for their stimulant use disorder. A range of treatment options should be offered and made available when people feel ready. Ideally, services can be brought to where people live or receive care, as navigating the treatment and health care systems can be a huge barrier.
AID: Prevent overdose deaths and reduce the harms of drug use
Overdose response education and naloxone are essential strategies to help people who use drugs stay alive and reduce negative health risks of using unregulated drugs. Overdose prevention can also catalyze communities to integrate other strategies:
- Naloxone distribution to people who may have or witness an opioid overdose
- Education on opioid overdose and safer use
- Community-based drug checking services
- Post-overdose follow-up care
- Distribution of safer drug use supplies
- HIV and hepatitis C (HCV) testing and treatment
- Education on short- and long-term impacts of stimulant use
CARE: Support the health of people at risk for overdose and/or working on their recovery
People who are actively using substances or in various phases of recovery, some of whom continue to use substances, likely need multiple services to address these needs, including:
- Medical care
- Housing supports
- Employment supports
- Mental health care
- Legal help
- Case management
- Alternatives to incarceration for drug-related crimes
CONNECT: Strategies to improve connections to care and services

Navigating health and treatment systems can be challenging. Easy and continued connections can happen through multiple approaches:
- Care navigation, often staffed by peers
- Community education and stigma reduction
- Education for providers who interact with people at risk of overdose within a range of settings (e.g., healthcare, behavioral health, housing, outreach, emergency services, law enforcement, corrections)
- Support and education for friends and family of people with OUD or at risk of overdose
Emerging strategies
While not available or even legal in many places in the United States, interventions like these are showing promise in other countries:
- Overdose prevention centers where people can consume drugs under medical supervision
- Safer supply distribution
Practices with limited effectiveness
Some long-standing practices may, in fact, increase a person’s risk for overdose. They can also make it harder to start or stay engaged with services:
- Inpatient/outpatient treatment or detox as standalones without buprenorphine or methadone These treatments without buprenorphine or methadone can lower someone’s tolerance and increase their risk for overdose.
- Lengthy wait times and assessments for SUD treatment
- Limited hours, distant locations, and rigid program rules
- Requiring, rather than offering, counseling as part of treatment for OUD
- Discontinuing SUD treatment or mental health care if someone continues to use drugs or starts again

Specific groups of people are dying from overdose at disproportionate rates in Washington State (or have seen recent increases). To have the maximum impact on mortality as quickly as possible, these populations need priority attention:
- People who use non-prescribed/illegal/unregulated substances
- People with OUD and/or stimulant use disorder
- People who recently survived an overdose or emergency related to substance use
- People in jail or prison (or who have left recently)
- People living unhoused
- People in permanent supportive housing
- Pregnant and parenting people with SUD
- Racial/ethnic groups experiencing high rates of overdose deaths (e.g., American Indian/Alaska Native/African American)
- Youth and young adults
These individuals can be reached through diverse settings such as:
- Health care
- Hospitals, emergency departments, primary care clinics, pharmacies
- Emergency medical services (EMS)
- Harm reduction programs
- Criminal legal system
- Jails, prisons, drug courts, juvenile detention, probation, parole programs
- Behavioral health programs
- Public health programs
- Social services
- Schools and organizations that serve youth
- Community organizations
- Housing support programs
- Homeless outreach programs

At the end of this document is a checklist you can use to guide your planning efforts. Follow these steps to create a holistic plan:
- Review your community’s data, including overdose deaths, hospitalizations, and treatment.
- Identify the resources and partners in your community.
- Set priorities based on input from people at risk of overdose and other stakeholders.
- Select evidence-based strategies (or promising practices) in each domain of the response continuum
- Choose evaluation metrics to measure the impact of your strategies.
- Regularly review your evaluation metrics and local data. Revise strategies as needed.
Evaluation metrics
Data can help identify which groups are currently most affected or where interventions are likely to have the highest impact. Common evaluation metrics include:
- Number of people receiving services at harm reduction programs
- Number of EMS calls for overdose
- Overdose deaths and hospitalizations
- Number of providers/clinics prescribing buprenorphine
- Number of people receiving buprenorphine or methadone
- Naloxone kits distributed to specific populations or in specific settings
- Jails and prisons providing medications for opioid use disorder (MOUD)
- Perspectives of people who use drugs from surveys and interviews on care needs, the appropriateness and quality of care, and access barriers.
Resource: Most States Already Collect Data That Can Help Improve Opioid Use Disorder Treatment: When used to inform policy, this information can increase access to care, save lives. Pew Charitable Trusts
Care Cascade Analysis
Some communities have used data to better understand how people enter and navigate systems such as healthcare or criminal justice. These data can help identify where people who have experienced or died from an overdose may have been served in the prior year. This can help focus interventions or identify dangerous transitions in care. Find helpful tips here: Cascade of care approach to treatment for OUD.
If you don't have these data, bring together diverse stakeholders across the care continuum to review local examples to see where care initiation, referral, and retention went well or did not.
Two examples of a Care Cascade Analysis from King County are:
- Integrating Data to Better Understand Fatal Overdoses and Service System Engagement: DCHS Data Insights Series
- Evolution of a Post-Overdose Outreach Program in King County, Washington: Lessons Learned Through Continuous Quality Improvement
Resource: Development of a Cascade of Care for responding to the opioid epidemic. American Journal of Drug and Alcohol Abuse

Essential and innovative programs that blend strategies include:
Syringe services programs (DOH): These provide safer injection and smoking supplies, HIV and HCV testing, and referrals to essential services. They are essential partners in distributing naloxone and overdose response education and distribute a large proportion of naloxone in Washington State. Some also provide low-barrier buprenorphine, wound care, and other medical care.
Primary prevention + harm reduction for youth (YouTube): Education for high school and college students should include: messaging about the risks of drugs, strategies to avoid using, and ways to use more safely if they do use.
Health engagement hubs (pdf, HCA): These “serve as an all-in-one location for low-barrier medical, harm reduction, behavioral health, and social services for people who use drugs” as defined by the Washington State Health Care Authority.
Other low barrier health programs: Low-barrier programs offer harm reduction supplies, health care, mental health referrals and care management, and medications for opioid use disorder in one location. These include low barrier opioid & stimulant use disorder services (UW ADAI).
Post-overdose response centers (DESC): After an overdose, people are taken to an overdose recovery center where they can rest and have access to buprenorphine and methadone if desired.
MOUD and naloxone in jails and prisons (pdf, HCA): People leaving jail or prison are at very high risk for overdose upon release. Providing buprenorphine in jails and also naloxone upon release can help reduce this risk.
Buprenorphine administered in the field (YouTube): Buprenorphine delivered to people after an overdose reversal with naloxone by the Seattle Fire Department. Another example is Downtown Emergency Services Center providing long-acting injectable buprenorphine to unhoused people and offering referrals for follow-up.
King County Telebup Hotline (UW): Hotline to connect people to three days of buprenorphine and referrals for longer-term access.
Comprehensive medical care for those using opioids/and or stimulants: Opioids and Stimulants: A Guide for Healthcare Providers from the University of California San Francisco.