“I Think One Enhances the Other”: Use of Harm Reduction & Drug Treatment Among Participants of Syringe Services Programs
Alison Newman, MPH; Teresa Winstead PhD, MA; Leif Layman, MPH
Full report | Participant summary | Webinar recording
Key Findings
- Interviews were conducted with 27 participants of three syringe services programs (SSPs) in WA State; all had recent experience with substance use disorder (SUD) treatment.
- Participants had used both SSPs and SUD treatment, sometimes concurrently. SSPs were often important access points for harm reduction services before, during, and/or after SUD treatment.
- The positive aspects of SSPs for participants included their easy access, friendly staff, and availability of supplies to meet basic needs and reduce health risks of drug use.
- The benefits of SUD treatment for participants included reduced drug use, better coping skills, and improved quality of life. However, participants also reported challenges in accessing or staying in treatment or finding programs that were a good fit.
- Most interviewees valued access to both harm reduction and SUD treatment concurrently, though some reported challenges using these services simultaneously.
- More than half the participants were interested in receiving treatment at an SSP due to the easy access and supportive staff.
Background

People who use drugs access different types of services to manage their health and substance use. These can include medical and mental health care, substance use disorder (SUD) treatment, and harm reduction services, most often provided by syringe services programs (SSPs)*. SUD treatment can include detox services, inpatient/outpatient treatment, medications prescribed for opioid use disorder (e.g., methadone, buprenorphine, naltrexone) or recovery support groups.
SSPs provide education, materials, and services to reduce risks of illicit drug use (e.g., sterile syringes and/or smoking equipment, naloxone, wound care supplies); address other health needs (e.g., nicotine replacement therapy, contraception, condoms); or fill basic needs (e.g., tents, food, clothing). Services and supplies vary by program, but all SSPs offer referrals to local services and SUD treatment. Learn more about WA State SSPs here.
Traditionally, the realms of harm reduction and drug treatment have often been seen (by providers and individuals) as siloed and mutually exclusive, given their different roles and orientations on abstinence. For many people who use drugs, however, these two worlds are often less distinct and may even overlap at times. This study aimed to understand the range of SSP participant perspectives about their use of harm reduction services and SUD treatment.
*“Syringe services programs” (formerly known as “needle exchanges”) provide education, materials, and services to support safer use of illicit drugs. From their inception, these programs have focused on injection drug use. But many now also provide supplies for safer smoking of drugs to engage people who do not or have never injected drugs. Because of this broader reach, some SSPs prefer to call themselves “harm reduction programs“ or “harm reduction centers.” For consistency, this report uses the term syringe services programs.
Methods
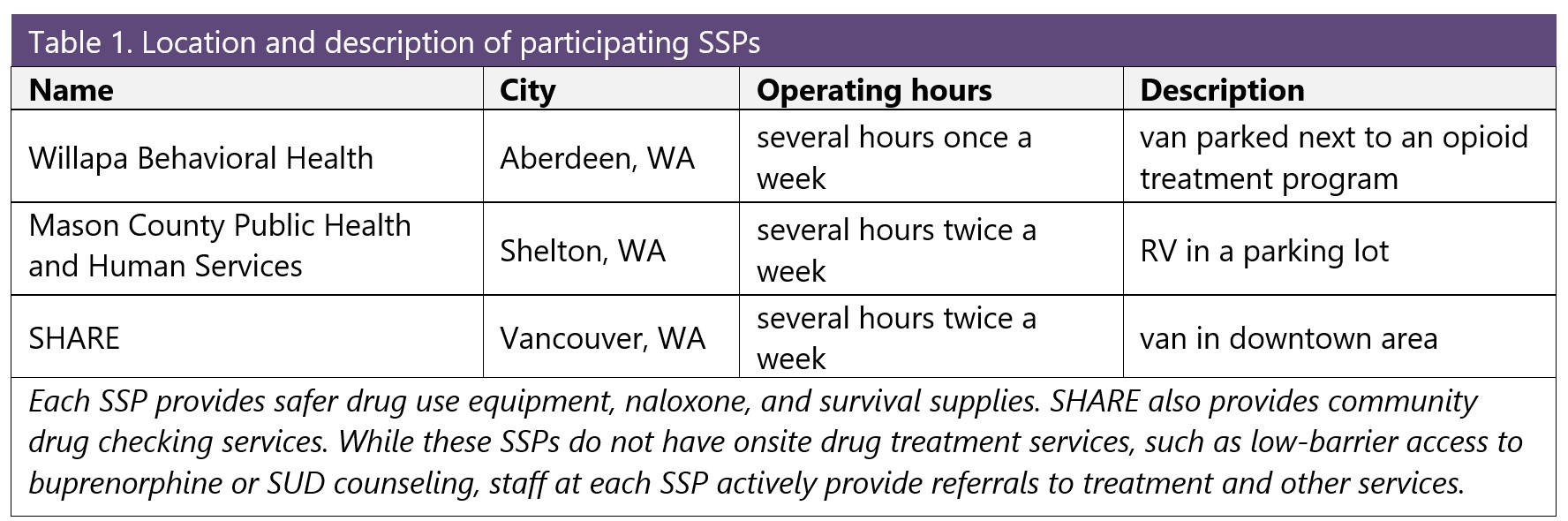
This descriptive study used qualitative interviews to understand experiences and perspectives of participants using both harm reduction services (at SSPs) and SUD treatment. Approval for this study was obtained from the University of Washington Human Subjects Division. Project partners included three SSPs in WA State that were selected for geographic variability and because they had not previously been involved in qualitative interviews with our team (Table 1).
Interviews were conducted during regular SSP hours in Fall 2024. SSP participants were eligible if they:
- had accessed SUD treatment in the last two years.
- had used non-prescribed opioids or stimulants in the past week.
- were at least 18 years old.
- spoke English.
“SUD treatment” was defined as any use of detox, inpatient or outpatient treatment, medication prescribed for opioid use disorder (i.e., methadone, buprenorphine, naltrexone) or recovery support/12-step groups.
Semi-structured interviews were completed after verbal informed consent was obtained. Interviews were recorded and transcribed by a HIPAA-compliant transcription service. Rapid qualitative analysis was conducted using transcript summaries and team-based thematic analysis (Hamilton, 2013; Hamilton et al., 2019). MaxQDA software (Verbisoftware 2022) supported the initial summary process. Data visualization was conducted in the R Language and Environment for Statistical Computing (R Core Team 2025) with the ggplot2 package (Hadley Wickham).
Results
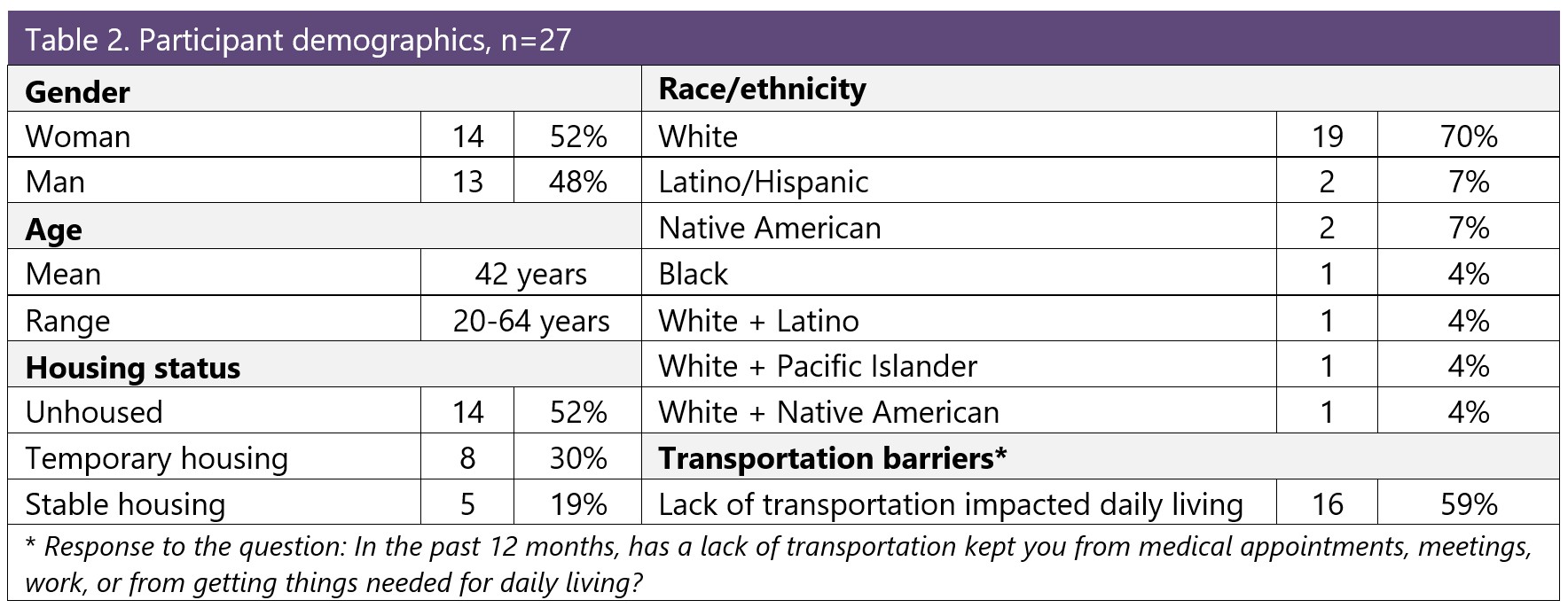
Twenty-seven interviews were conducted (Aberdeen: 15, Shelton: 5, Vancouver: 7). The majority of respondents were white (70%), with some participants identifying as Black, Latino, Native American, or Pacific Islander. Slightly over half of participants (52%) were unhoused, and about a third lived in a temporary housing situation. The gender of participants was evenly split between men and women. The average age was 42, with an age range of 20-64 years old (Table 2).
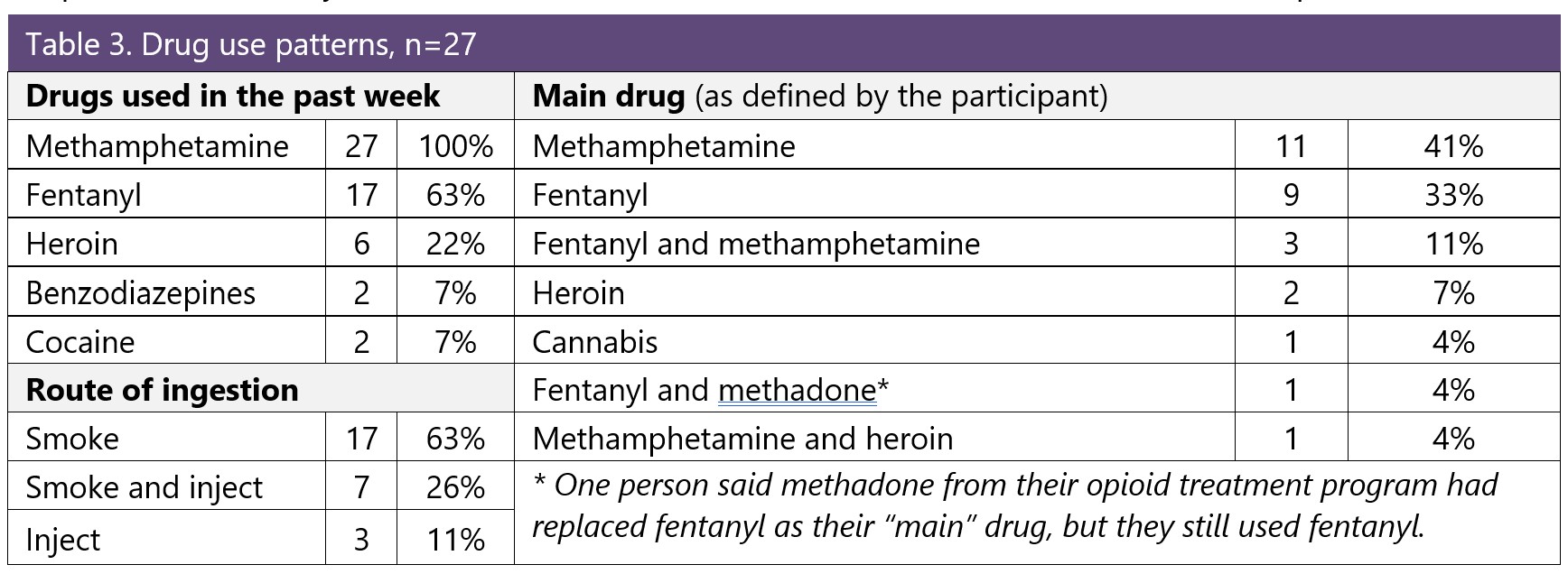
All participants reported using methamphetamine in the past week, and two thirds reported using fentanyl in the past week (Table 3). Some had used heroin in the past week but said this was less frequent than fentanyl because heroin was less available. A few had used benzodiazepines or cocaine.
A third of participants reported using only methamphetamine, and no other drugs, in the past week. Conversely, all of those who had used fentanyl in the past week also reported using methamphetamine. Participants primarily identified methamphetamine (41%) or fentanyl (33%) as their “main drug,” while 11% considered both as their main drugs. The majority of people currently smoked their drugs as their only route of administration. Fewer people also injected (or only injected) drugs currently.
Participants were asked to describe a timeline of when they first used a stimulant or opioid, first tried an SSP, and first tried SUD treatment. Figure 1 shows that the timing and sequencing of these first-time events varied across participants. Some people had engaged in harm reduction or treatment services early in their use; others had substantial gaps from when they started to use drugs until they first accessed an SSP or treatment program. Although all participants had used SUD treatment in the past two years (an eligibility criterium), 19% (n=5) of participants reported being currently in treatment, and 26% (n=7) reported using some form of SUD treatment within the calendar year.
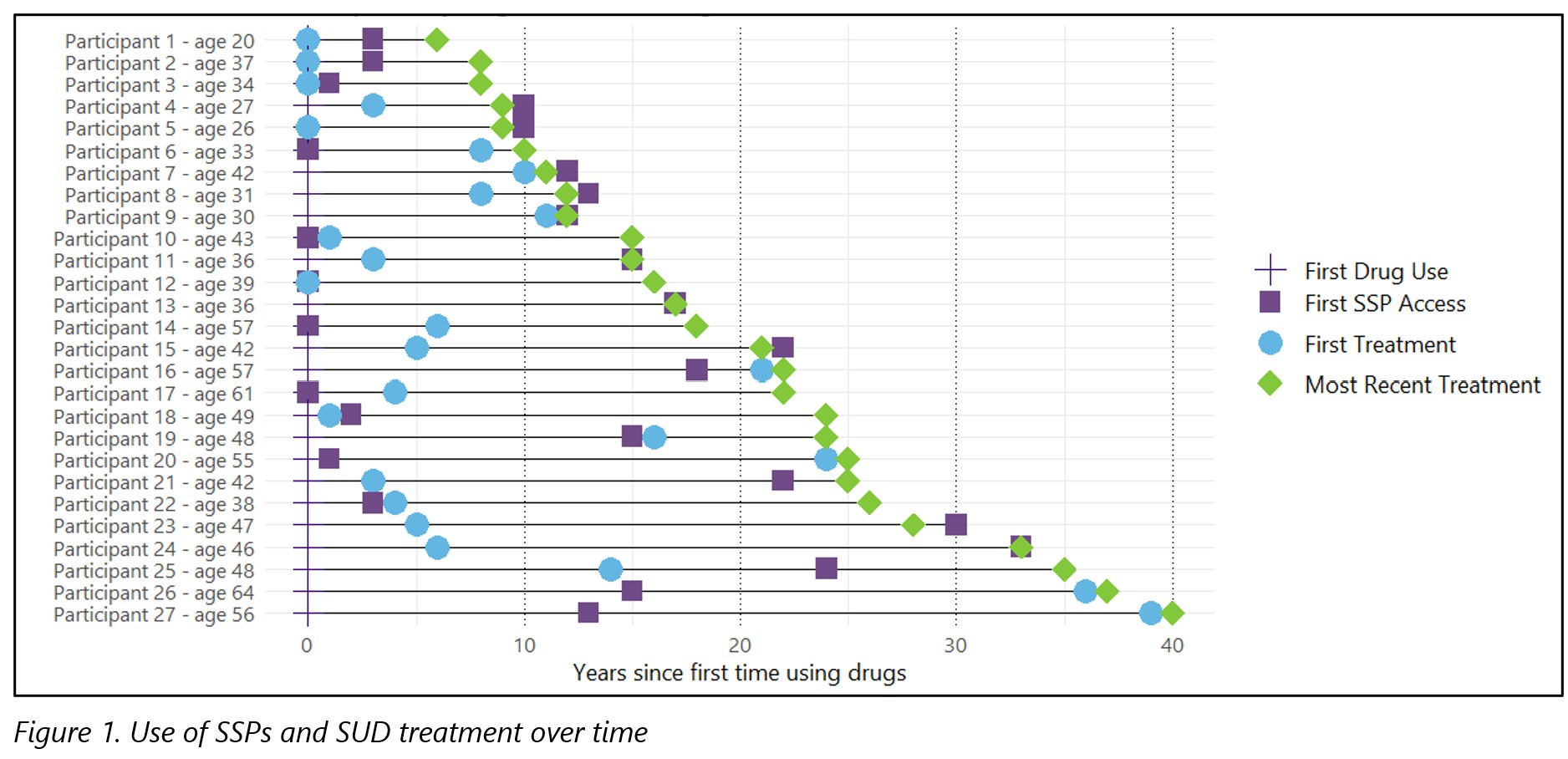
Ten participants (37%) had used an SSP prior to SUD treatment; three (11%) had started to use an SSP and SUD in the same year; and 14 (52%) had tried SUD treatment prior to using an SSP.
Many participants reported using services at their current SSP for years or decades, although some began accessing services as recently as 2024.
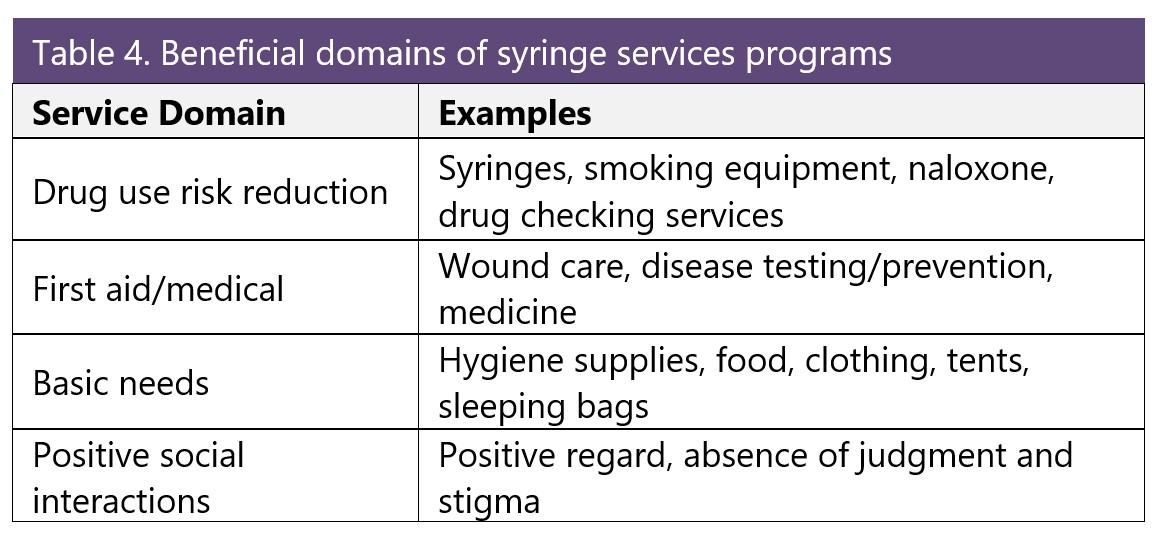
Overall, participants viewed their SSP favorably as a unique and significant service that had a positive impact on their lives and the community. Participants described multiple benefits from services at SSPs which fell into four general domains: drug use risk reduction, first aid/medical, basic needs, and positive social interactions (Table 4).
Regarding wound care, participants noted that medical supplies (e.g., bandages, gauze, antibiotic ointments) were expensive and hard to get. Therefore, access to these wound care supplies at SSPs was hugely beneficial, and in some cases, even life-saving:
“I'm pretty sure that if it wasn't for this exchange [SSP] right here doing what they're doing, I would either be dead or I would not have legs because they keep me in my medical supplies so I can keep my wounds clean. I'm sure I would have been dead because this has killed me twice already ... this exchange has been really wonderful.”
Participants appreciated receiving food, water, clothing, hygiene kits, and outdoor supplies (e.g., sleeping bags, tents) and noted these supplies were of great value to their quality of life and well-being. They also identified positive, judgment-free interpersonal interactions as one of the most valuable aspects of using the SSP and often different from interactions with the public or in healthcare.
“The workers are always really nice and helpful, and they're always there with a smile on their face and there to help us out and give us our supplies when we need them. It's nice to have people like that because there's not a lot of people around here that are like that, that are giving and kind.”
“Just that I guess I get some positive interaction with somebody, where people aren't demeaning or put off a way that they're judgmental or—just positive human contact … it's one of the greatest things about dealing with the people, here.”
Many participants reported that they would continue to engage with harm reduction services in the future, and for some, even if they stop using drugs.
Suggestions for improvement

Some participants suggested improvements and additional services for SSPs such as:
- Expanded hours of operation
- Flexible service models (e.g., home delivery, mail order)
- Easier to access location
- Additional hygiene services
- Safer smoking supplies (at programs that did not already provide them)
- Relapse prevention supports
- Access to bus passes, gift cards, and other supplies to help cope with homelessness

People reported using several forms of SUD treatment since they started using drugs, particularly in the last two years. These included:
- Detox services
- Outpatient and/or inpatient treatment
- Medications for opioid use disorder (MOUD)
- 12-step/recovery support groups
Two-thirds of participants reported trying MOUD at least once. Several people discussed having tried SUD treatment (outpatient or inpatient) multiple times in the past, including having tried the same type of treatment more than once. One young person described having tried SUD treatment seven times in the past two years. While some people said they were able to achieve long periods with no or reduced drug use, others reported that they continued some level of substance use even while in SUD treatment (most often while on MOUD).
Motivations for SUD treatment
Participants were motivated to try SUD treatment to stop or control their drug use, often in order to improve quality of life. Motivations included: not wanting to die/concerns about overdose; to improve or save their health; to stay out of jail; or to be there for family or regain custody of their children.
“I'm 20. I have so much time in my life that I don't want to waste out here. I don't know. It's not worth it, chasing something that's never going to satisfy you. So I'm just tired of this lifestyle. I'm tired of these people. And I'm either going to end up in the grave or behind bars, and I'm not really trying to go to jail, and I don't want to die, so.”
A few people reported they started SUD treatment to primarily satisfy drug court or housing program requirements, rather than from a personal desire to stop using.
Benefits of SUD treatment
Several people spoke about positive experiences with SUD treatment staff, describing them as supportive, welcoming, or helpful. Other positives described were easy access due to location or transportation support. Others described the benefits of group counseling or accountability. A few people felt their health improved after a break from drug use, or that stopping drug use was essential to staying alive. Participants’ positive experiences with MOUD varied, but there was wide support for MOUD as a treatment that “worked well” to help decrease drug use and increase other positive elements of their lives.
“I just needed to-- well, I mean, I wanted to change my internal dialogue. I have this small voice in my head telling me these things that I thought were…then I went to treatment, and everything that I was speaking was confirmed by somebody really smart.”
Negative experiences with SUD treatment often reflected challenges with rigid treatment environments or rules:
“They’re like, 'You get a dirty UA you're getting kicked out.' and I'm like, 'Shit'… It was terrifying.”
Most participants identified some barriers to starting or continuing SUD treatment, including: fear of withdrawal or stopping drugs, life challenges, self-motivation, health insurance, transportation, and program requirements, such as requiring counseling sessions with methadone dosing or completing detox first. Other barriers were medical issues or being sent to jail or prison.
“I had to start out going every week, and I was doing two and a half Suboxone [strips] daily. And then when I was so far along, then I just had to go every month. But then once I started-- I think I was at every three months. Then I started slacking, and then I just relapsed. I had to go to ____. So then my car broke down and then lost transportation. Had to take the bus. So then I just stopped going.”
Suggestions for improvement
Participants shared various recommendations for how to improve their treatment experience. These included more flexible options for treatment, both in types of services offered, as well as modes of access, such as lower-barrier or virtual. Others spoke about wanting a “one-stop-shop.” A few people spoke about the importance of connection and support after leaving SUD treatment.
Conclusions
- Participants appreciated easy access to SSPs, positive interactions with non-judgmental and caring staff, and the availability of essential resources that were hard to get otherwise.
- Benefits of SUD treatment included help to reduce or stop drug use, better coping skills, and reconnection with children/family. Many felt buprenorphine or methadone provided stability.
- Although harm reduction and SUD treatment have different approaches and intentions, the majority of participants felt these programs could be complementary; using both harm reduction and SUD treatment programs had substantial benefits.
- Participants expressed broad support for the cross-pollination of SUD treatment and harm reduction services. This included support for providing both types of services in the same location and for providing education about both types of services in different programs.
- People expressed interest in obtaining treatment and other services at the SSP because of the lower-barrier access.
- People endorsed expanding access to low-barrier and flexible programs where supportive staff could provide holistic care and offer supplies to meet basic needs.
Limitations
The majority of people we spoke with were unhoused, and their perspectives may not be representative of everyone who uses drugs. Our interviews did not ask about other services such as medical care, housing, legal aid, or other supports, although those issues arose frequently. Interviews were conducted only at vehicle-based SSPs where cohoused SUD services are not available. Perspectives may be different among participants of SSPs that do have onsite SUD treatment services.
The interviews collected for this study were gathered using purposive, non-random sampling and as such are limited in terms of their generalizability. We talked exclusively to people who were currently using SSP services, so the possibility of documenting negative experiences with SSPs, including discontinuation of SSP use, was limited by design. In addition, alternative perspectives from people currently in SUD treatment about their experiences using harm reduction services/SSPs was not a part of this study. Further research on these additional perspectives could contribute meaningfully to this area.
Acknowledgements: Thank you to the syringe services program participants who shared their time, expertise, and experiences with us. Your insights and knowledge are essential to guide the work to reduce improve the health of people who drugs.
Thank you to the syringe services programs who partnered with us on this project: Mason County Public Health and Human Services, SHARE Vancouver, and Willapa Behavioral Health. These interviews were possible thanks to the trust and positive relationships you have with your participants. We appreciate the work you do to keep people alive.
WA Health Care Authority funded this project and had no editorial role.